Cobra Election Form Letter
Fillable Cobra Letter 2020 Fill Online Printable Fillable Blank Pdffiller
Blank Cobra Election Forms Fill Out And Sign Printable Pdf Template Signnow
Cobra Notice Fill Out And Sign Printable Pdf Template Signnow
Sample Cobra Election Notice

Election Form Sample Fill Online Printable Fillable Blank Pdffiller
Model Cobra Continuation Coverage Election Notice Form Download Printable Pdf Templateroller
Cobra coverage election agreement i have read this form and the notice of my election rights.
Cobra election form letter. Under federal law you have 60 days from the date of the letter you received or 60 days from the date your health insurance coverage terminated whichever is later to choose your continuation coverage election. To elect continuation coverage you must complete the enclosed election form and return it to the cobra administrator according to the directions on the election form. Please complete and submit this form.
I understand my rights to elect continuation coverage and would like to take the action indicated below. First name last name. I understand that if i elect continuation coverage and i fail to pay any hra premium payment on time this coverage will terminate.
If you choose to elect extended coverage cobra you should use the election form provided later in this notice and submit it to the designated individual by the end of the 60 day election period specified on the election form. Cobra continuation coverage election form. Cobra ucc election notice.
Namedate of birthrelationship to employeessn or other identifier a. Before sharing sensitive information make sure you re on a federal government site. I we elect cobra continuation coverage in the enter name of plan the plan listed below.
Mail or fax completed health care fsa cobra election form to. To elect cobra continuation coverage follow the instructions and complete the cobra continuation coverage election form and submit it to hfs cobra. Office of group benefits flexible benefits administration post office box 44036 baton rouge louisiana 70804 225 925 4860 fax this health care fsa cobra election form must be completed in writing and mailed or faxed to the department and address specified above.
Read the important information about your rights included in the pages after the election form. The completed election form must be postmarked no later than 60 days from the date of this letter or the loss of your coverage whichever is later. You must elect coverage no later than the date indicated in the election form.

Model Cobra Continuation Coverage Election Notice Alexander Street A Proquest Company
Model Cobra Continuation Coverage Election Notice Goodwin

Cobra Continuation Coverage Election Notice Template Download From Human Resources Policies And Procedures
Cobra Notification And Election Letter
Cobra Continuation Coverage Election Notice Iuoe Local 4 Benefit

Initial Cobra Notice Agc Health Plans Nw

Cobra Appeal Fill Online Printable Fillable Blank Pdffiller

Insurance Benefits After Termination
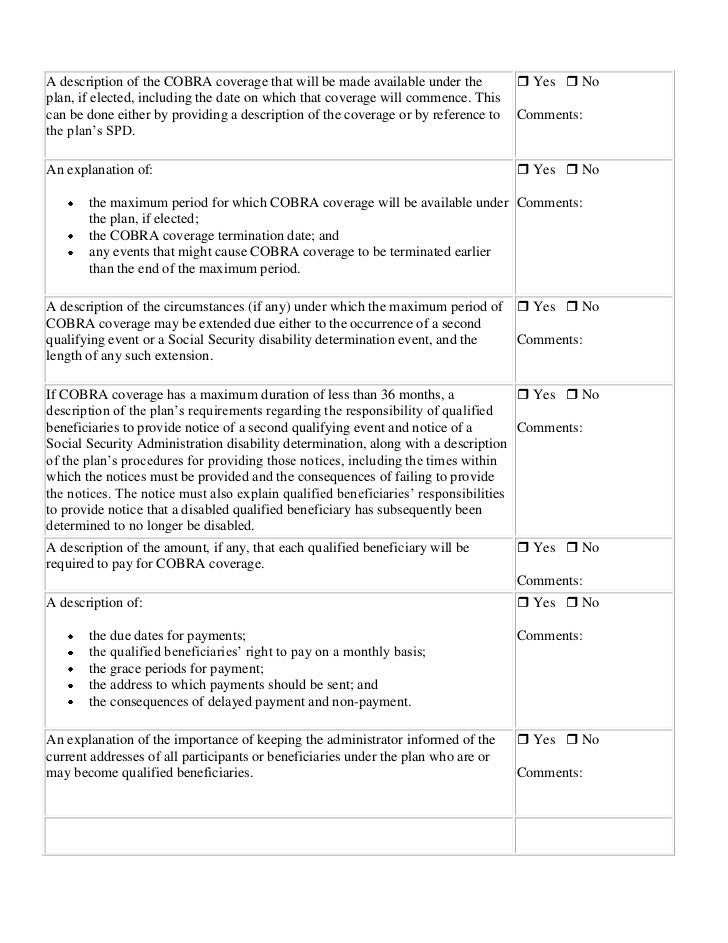
Cobra Qualifying Event Notice Checklist

Business Separation Agreement Template In 2020 Separation Agreement Separation Agreement Template Agreement

Offering Of Cobra Continuation Coverage Form Fill Online Printable Fillable Blank Pdffiller
