Election Form For Cobra Continuation Coverage
Fillable Cobra Letter 2020 Fill Online Printable Fillable Blank Pdffiller
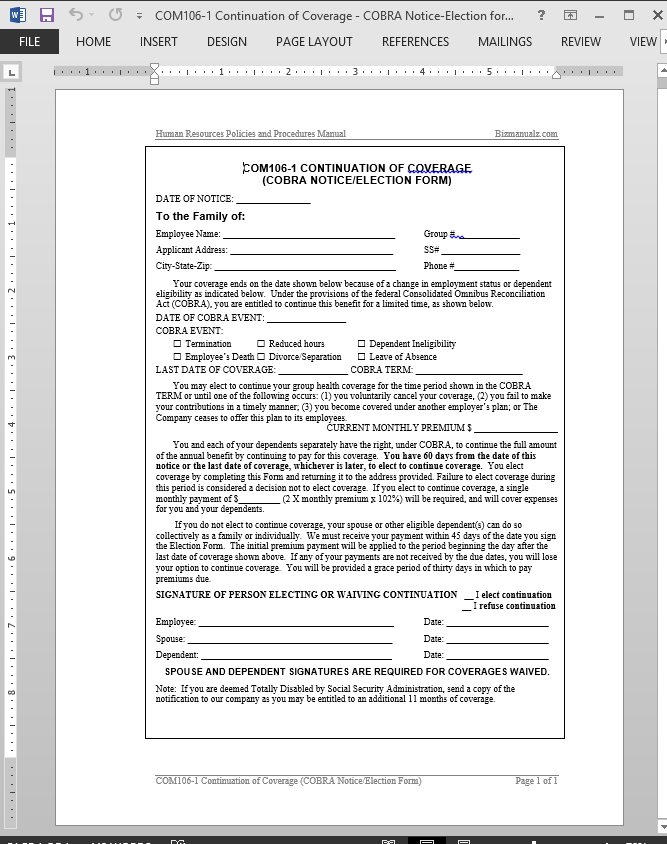
Cobra Continuation Of Coverage Request Template
Model Cobra Continuation Coverage Election Notice Alexander Street A Proquest Company
Blank Cobra Election Forms Fill Out And Sign Printable Pdf Template Signnow
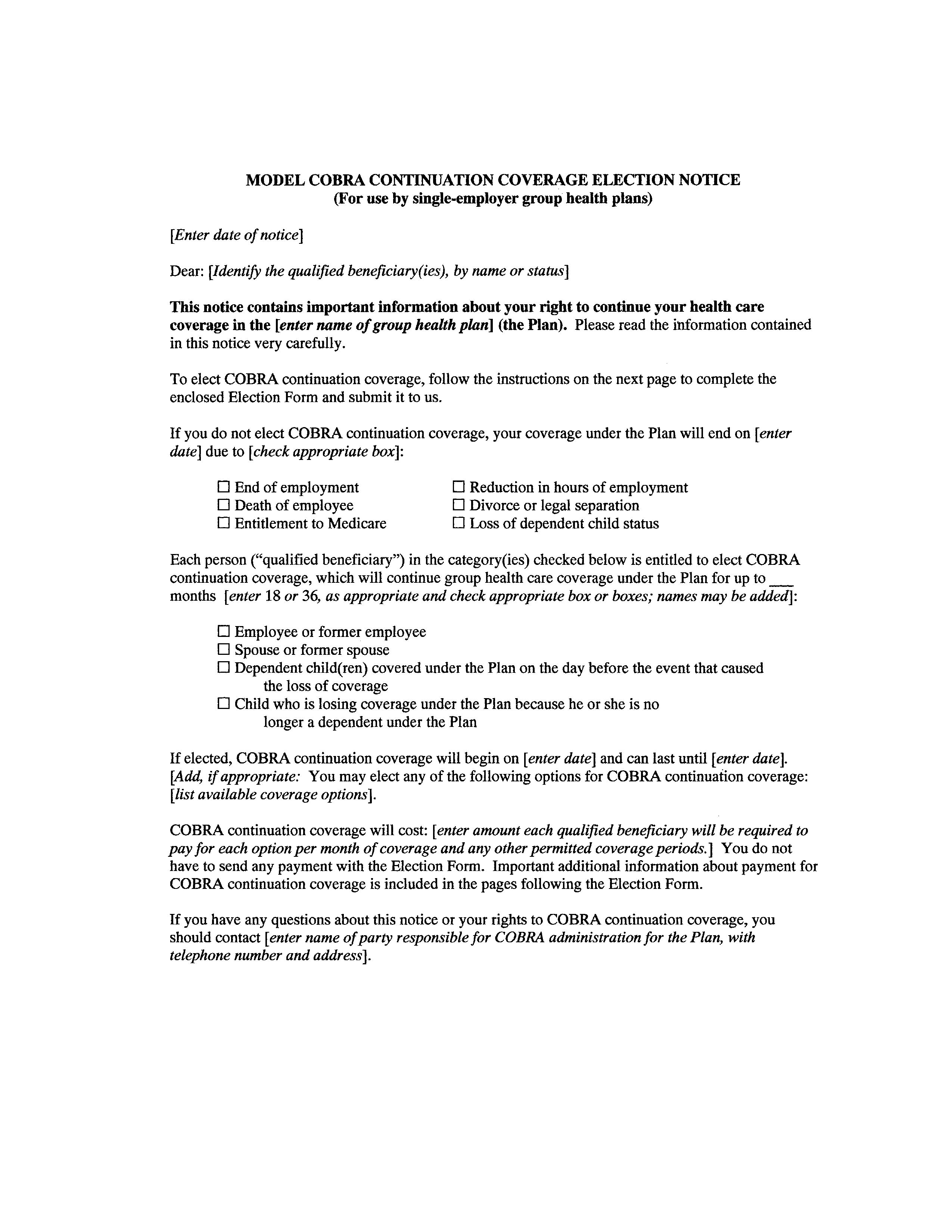
Sample Cobra Election Notice

Election Form Sample Fill Online Printable Fillable Blank Pdffiller
Cobra continuation coverage election form.
Election form for cobra continuation coverage. The return date should be 60 days from the plan termination date or 60 days from the date of notice whichever is later. This form is to be filled out using information from the cobra continuation coverage election notice. This election form contains important information about your right to continue your health care coverage in the group health plan identified above the plan as well as other health care coverage alternatives that may be available to you through the.
If all the qualified beneficiaries reside at the same address the plan administrators may either include separate election notices for each qualified beneficiary in a single mailing that is addressed to both the employee and spouse or send a single notice that clearly identifies all qualified beneficiaries covered by the notice and explains each person s separate and independent right to elect cobra continuation coverage. To elect cobra continuation coverage complete this election form and return it to us. This notice must be sent to the plan participants and beneficiaries by first class mail or hand delivered not later than 14 days after the plan administrator receives notice that a qualifying event occurred.
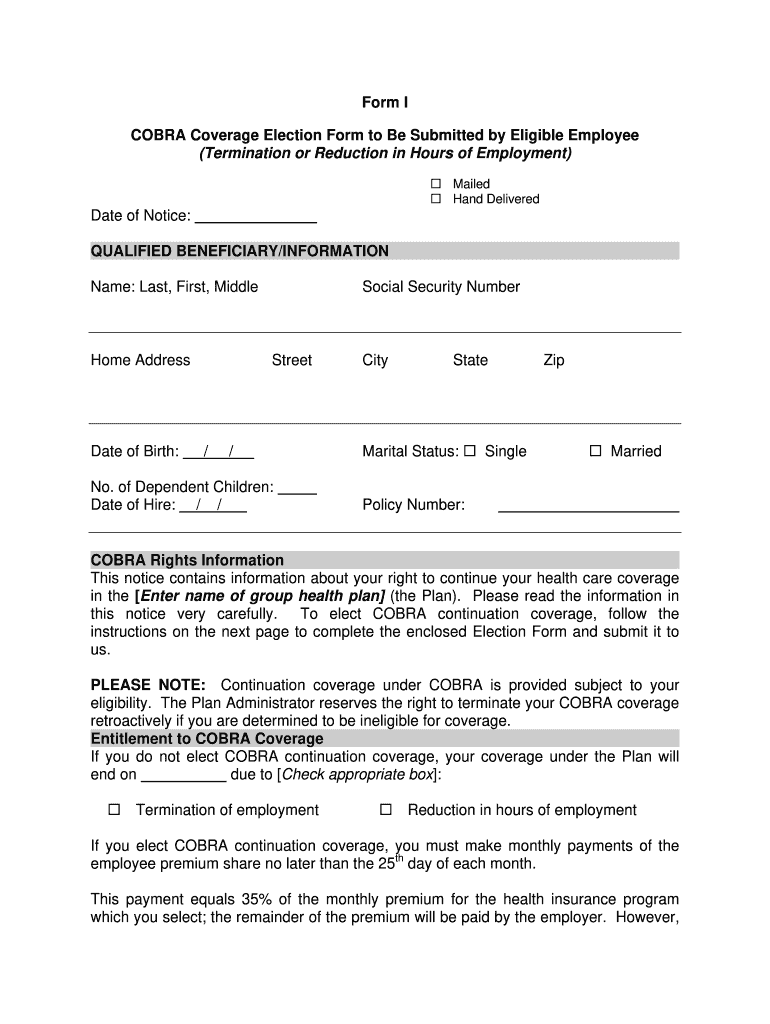
1 complete sign and date this cobra continuation coverage election form and make a copy for your. To elect cobra continuation coverage complete this election form and return it to your former employer. Cobra continuation election form iowa wesleyan university 00053527 7000 date of notification.
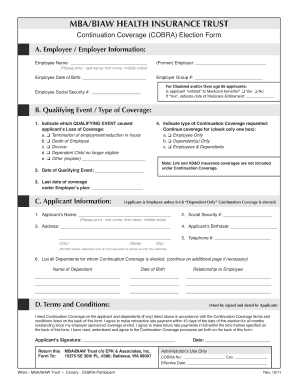
Please follow the election procedures listed below. Used by members to provide samaritan health plans current mailing addresses for all cobra continuation coverage members. Admac001 10 14 1 cobra continuation coverage election form refer to instructions attached to this form 700 bishop st.
Section ii to be completed by cobra enrollee or guardian. Under federal law you must have a maximum of 60 days after the date of this notice or from the first date of no coverage whichever is later to decide whether you want to elect cobra continuation coverage under the plan. 700 honolulu hi 9681 3 section i notification and form completion to be completed by the plan administrator 1.
Cobra continuation coverage election form. Send completed election form to. Used by members to enroll in cobra continuation coverage cobra address notification form.

Cobra Continuation Coverage Election Notice Template Download From Human Resources Policies And Procedures
Https Healthplans Providence Org Media Files Providence 20hp Pdfs Producers Documents Cobraform Pdf
Fillable Online Cobra Election Form Epk Benefits Group Insurance Programs Fax Email Print Pdffiller
Free 11 Employee Election Forms In Pdf Ms Word
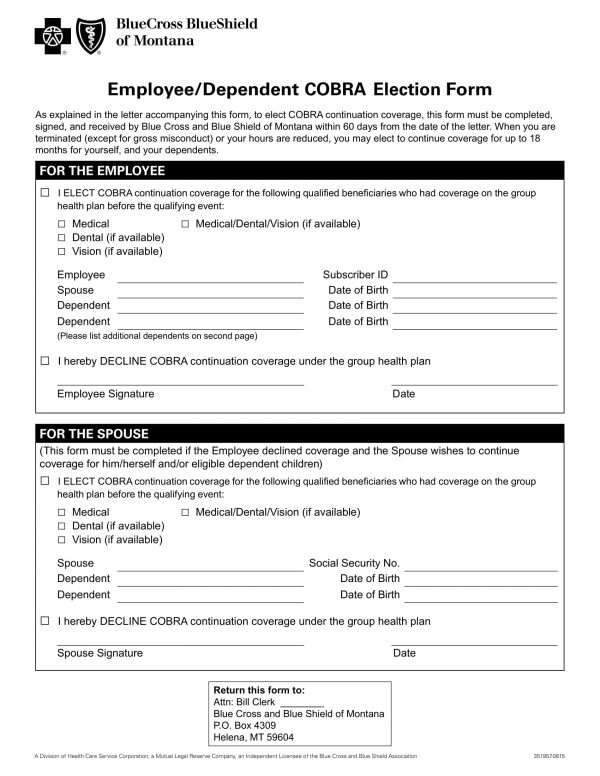
Https Www Bcbsal Org Rapidresponse Pdf Mkt 53 Pdf

Cobra Printable Cobra Snake Head Stl File Stlfinder Estele Abimillepattes Com
Model New York State Continuation Coverage Election Notice 2020 Fill Out And Sign Printable Pdf Template Signnow
Https Www Hca Wa Gov Assets Pebb Sebb Continuation Coverage Cobra Election Change Form 20 0060 2020 Pdf
Https Www Hca Wa Gov Assets Pebb 50 245f Pebb Continuation Coverage Cobra Election Change Form 2020 Pdf

Benefit Election Form Template Word Fill Online Printable Fillable Blank Pdffiller
Https Hr Umich Edu Sites Default Files Cobra Faq Pdf